
Myopia or shortsightedness is a common vision problem affecting a growing number of children worldwide.
The exact cause of myopia is multifactorial, involving a combination of genetic and environmental factors. Genetic predisposition plays a significant role, especially if both parents are myopic. However, environmental factors such as excessive near work, prolonged screen time, and limited outdoor activities also contribute to the development and progression of myopia.
In myopia, the eyeball tends to elongate more than normal, causing light to focus in front of the retina instead of directly on it. This results in blurry distance vision.

High myopia, if left unmanaged, can lead to various complications in adulthood. These complications may include:
High myopia is associated with an increased risk of retinal detachment. The elongation of the eyeball can cause the retina to thin, making it more susceptible to tearing or detaching. Retinal detachment is a serious condition that requires immediate medical attention.
High myopia is a risk factor for the development of age-related macular degeneration (AMD) in later years. AMD can result in the loss of central vision, impacting activities like reading and recognizing faces.
Individuals with high myopia may have an elevated risk of developing glaucoma, a condition characterized by increased pressure within the eye. Glaucoma can lead to optic nerve damage and gradual loss of peripheral vision.
High myopia may accelerate the formation of cataracts, clouding of the eye’s natural lens.





The Eyerising Myopia Management Device unit delivers red light at the right wavelength and intensity to gently stimulate blood flow in the ocular fundus to alleviate sclera hypoxia and control the axial lengthening that causes myopia.
Therapy involves looking into the device for 3 minutes of treatment, twice a day, 5 days per week, with a minimum of 4 hours between sessions. The device is controlled with a simple touchscreen and is suitable for children as young as 3 years of age.
The goal of myopia management is to control or stablise the progression (axial length elongation) and prevent to develop into high myopia. It depends on the age of your child. For younger children, they may need RLRL therapy for a longer time. For teenagers, it will be a shorter time. As they are becoming adults, the progression is slower naturally as well. We recommend to start the therapy for 2 years and decide if your child needs further treatment afterwards. The life service of the device is 5 years.
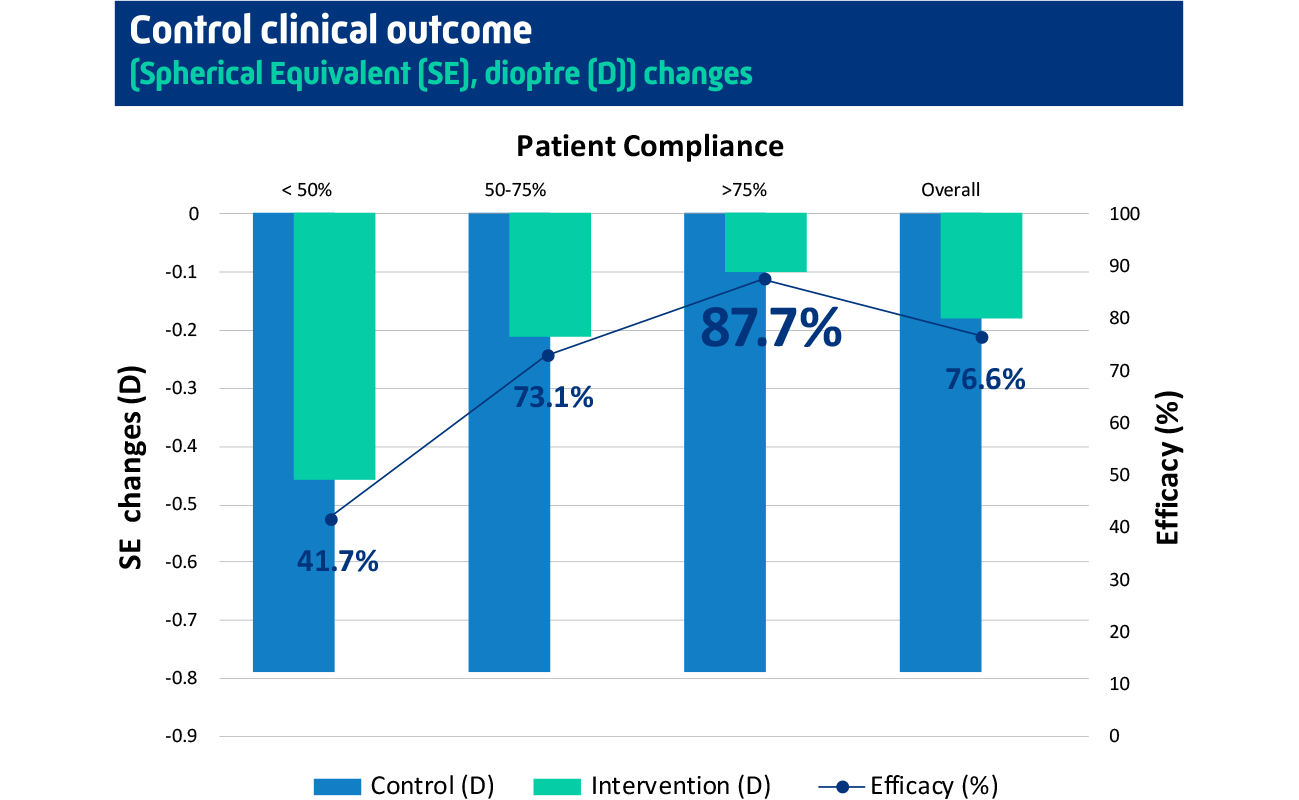
The child needs to use the device TWICE a day, 5 days a week, which means 10 times a week. It is really important to follow this guidance. Our clinical trial showed that higher compliance rate means higher efficiency results. When the compliance rate is more than 75%, the control efficiency is about 90%.
No, your child can use the device anytime during the day and any 5 days during the week. But to remember, there is at least 4 hours gap between two sessions on the same day. And we recommend using the device from Monday to Friday and taking the weekends off. In this way, it is easier to fit the treatment into their school schedule (once before school and once after school) and form a habit.
Once stops using the device, we recommend to get your child’s eyes checked routinely (every 6 months). From our clinical trial results, your child’s eyes will progress naturally. It depends on your child’s age, lifestyles and other multi-factors. Based on the routine check-up results, your child may require a longer period of RLRL treatment or other treatment, like low-dose atropine.
The common discomfort we observed is afterimage, which means the child can still see the red light after the treatment. But it will disappear within 3 minutes. We recommend the child close the eyes for 1 to 3 minutes after the treatments to avoid visual disturbances. With longer treatment, the duration of afterimage will get shorter and eventually disappear. If the afterimage is longer than 5 minutes, please stop using the device and contact the clinician for further advice.
If it is a short period of time (within one week). It is ok to skip a few sessions and go back to the routine after coming back home. But for a longer period, we recommend you bring the device with you. The device is very light and portal. It comes with a special package and great protection. It is like a small-size luggage that you can easily travel with.
Yes, your child needs to wear glasses to get corrected vision. Studies have shown that children are more likely to have a higher myopia progression rate when the vision is uncorrected.
Make sure your child takes off the glasses (single vision glasses, specially designed glasses or contact lenses) during the treatment session.
It is also mandatory to keep the eyes open during the 3-minute session. But your child can blink the eyes as normal.
To achieve good treatment results, the parent should help the child to adjust the interpupillary distance and make the two red dots merge into one dot. If it is not possible, make sure the red light achieves the brightest level.
Yes, RLRL can combine with Orthokeratology lenses, soft contact lenses (e.g. MiSight ) and specially designed glasses( e.g. Hoya Miyosmart). But RLRL cannot used in conjunction with atropine (e.g. Myopine). So please make sure your child stops using atropine for 2 weeks prior to the commencement RLRL therapy.
Yes, our clinical trial showed that the RLRL group had > 0.05 mm axial length shortening, which is the precision for the device and indicating the true shortening rather than measurement error in 39.8% of the participants at 1 month and 21.6% of the participants at 12 months.
Axial length is considered the ‘gold standard’ in assessing myopia control efficacy as it is more sensitive to detect myopia progression than refraction. Axial length is also a strong predictor for myopic pathology which allows clinicians to predict the children’s risk of associated disease for myopia. Subjective refraction is also an acceptable alternative.
Eyerising International is represented in Malaysia by Aionlabs Sdn Bhd, an authorised distributor of medical and pharmaceutical products.
Copyright © 2024 Eyerising®. All rights reserved.