
At last, there is a simple and effective myopia control therapy developed especially for children, guardians and practitioners. Using patented technology to deliver Repeated Low-Level Red-Light (RLRL) therapy, the Eyerising Myopia Management Device unit gently stimulates blood flow in the ocular fundus to alleviate sclera hypoxia and control the axial lengthening that causes myopia.
The device is a powerful addition to the clinician’s existing myopia toolkit, providing the potential for earlier treatment, additional patient treatment optionality and the potential for RLRL as a new adjunct therapy.^ The device monitors and shares patient compliance data with practictioners for use during follow-up examinations.
^ RLRL cannot be used in conjunction with atropine. Patients need to stop using atropine for 2 weeks and then start RLRL therapy.
Therapy involves looking into the device for 3 minutes of treatment, twice a day, 5 days per week, with a minimum of 4 hours between sessions. The device is controlled with a simple touchscreen and is suitable for children as young as 3 years of age.
The device is a powerful addition to the clinician’s existing myopia toolkit, removing tears and complications that limit compliance. It securely shares patient compliance data with practitioners, enabling superior follow-up assessment. It also sends reminders to the guardian when the patient misses treatment to maximise patient treatment efficacy.
Usable as a stand-alone therapy without eyedrops, lenses or complications. Or as a powerful adjunct to existing therapies for patients who are not responding to Ortho-k.
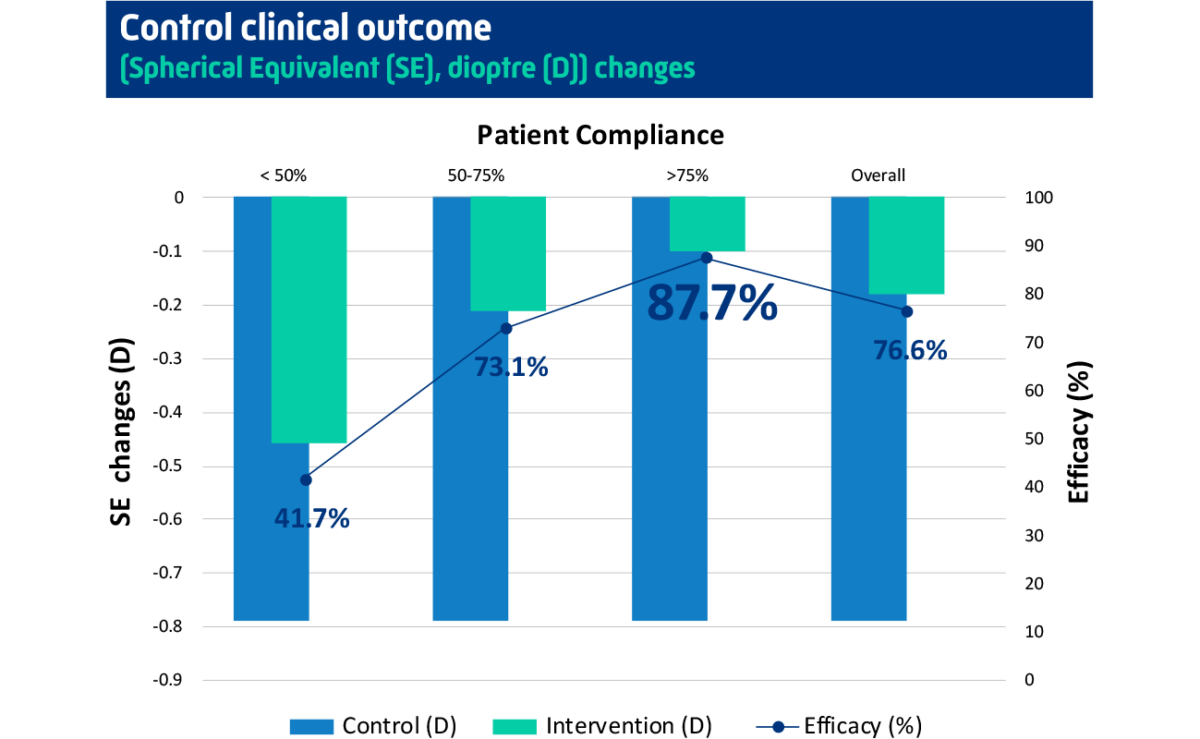
The device has been proven in published clinical trials to be effective in the treatment of myopia, dramatically slowing its progression by up to 87.7%.
The goal of myopia management is to control or stablise the progression (axial length elongation) and prevent to develop into high myopia. It depends on the age of your child. For younger children, they may need RLRL therapy for a longer time. For teenagers, it will be a shorter time. As they are becoming adults, the progression is slower naturally as well. We recommend to start the therapy for 2 years and decide if your child needs further treatment afterwards. The life service of the device is 5 years.
The child needs to use the device TWICE a day, 5 days a week, which means 10 times a week. It is really important to follow this guidance. Our clinical trial showed that higher compliance rate means higher efficiency results. When the compliance rate is more than 75%, the control efficiency is about 90%.
No, your child can use the device anytime during the day and any 5 days during the week. But to remember, there is at least 4 hours gap between two sessions on the same day. And we recommend using the device from Monday to Friday and taking the weekends off. In this way, it is easier to fit the treatment into their school schedule (once before school and once after school) and form a habit.
Once stops using the device, we recommend to get your child’s eyes checked routinely (every 6 months). From our clinical trial results, your child’s eyes will progress naturally. It depends on your child’s age, lifestyles and other multi-factors. Based on the routine check-up results, your child may require a longer period of RLRL treatment or other treatment, like low-dose atropine.
The common discomfort we observed is afterimage, which means the child can still see the red light after the treatment. But it will disappear within 3 minutes. We recommend the child close the eyes for 1 to 3 minutes after the treatments to avoid visual disturbances. With longer treatment, the duration of afterimage will get shorter and eventually disappear. If the afterimage is longer than 5 minutes, please stop using the device and contact the clinician for further advice.
Please submit an inquiry on the customer portal, our team will contact you as soon as possible.
Axial length is considered the ‘gold standard’ in assessing myopia control efficacy as it is more sensitive to detect myopia progression than refraction. Axial length is also a strong predictor for myopic pathology which allows clinicians to predict the children’s risk of associated disease for myopia. Subjective refraction is also an acceptable alternative.
If it is a short period of time (within one week). It is ok to skip a few sessions and go back to the routine after coming back home. But for a longer period, we recommend you bring the device with you. The device is very light and portal. It comes with a special package and great protection. It is like a small-size luggage that you can easily travel with.
Yes, your child needs to wear glasses to get corrected vision. Studies have shown that children are more likely to have a higher myopia progression rate when the vision is uncorrected.
Make sure your child takes off the glasses (single vision glasses, specially designed glasses or contact lenses) during the treatment session.
It is also mandatory to keep the eyes open during the 3-minute session. But your child can blink the eyes as normal.
To achieve good treatment results, the parent should help the child to adjust the interpupillary distance and make the two red dots merge into one dot. If it is not possible, make sure the red light achieves the brightest level.
Yes, RLRL can combine with Orthokeratology lenses, soft contact lenses (e.g. MiSight ) and specially designed glasses( e.g. Hoya Miyosmart). But RLRL cannot used in conjunction with atropine (e.g. Myopine). So please make sure your child stops using atropine for 2 weeks prior to the commencement RLRL therapy.
Yes, our clinical trial showed that the RLRL group had > 0.05 mm axial length shortening, which is the precision for the device and indicating the true shortening rather than measurement error in 39.8% of the participants at 1 month and 21.6% of the participants at 12 months.
For more details please visit the Science Hub.
Eyerising International is represented in Malaysia by Aionlabs Sdn Bhd, an authorised distributor of medical and pharmaceutical products.
Copyright © 2024 Eyerising®. All rights reserved.